Road Construction Alert: King County Metro construction is planned on Talbot Rd. S from July 27 - August 8. Hours of work will be Monday - Friday, 9 AM - 3 PM. This will impact traffic around the hospital and clinics. Please plan accordingly. See King County Metro's website for project details.
Update for Surgeons and Proceduralists
Dear VMC Surgeons and Proceduralists,
Last week, you received information and guidance regarding the current situation with elective procedures (copied for your information below.) Please continue to review your cases/procedures. We have the ability to perform procedures safely for both our patients and staff. Please schedule any patient procedures which may include imaging, lab, interventional procedures and surgeries that in your clinical judgment you believe would cause your patients harm if further delayed.
Between now and May 18, please use the dot phrases listed here to document your decision making with regard to harm. It should be placed along with your interval note If an interval note is not applicable to the service the patient is receiving, please document in an appropriate area of the clinical record. Also, please continue to share this information during your informed consent review with the patient.
Lastly, in preparation for May 18, our plan is to reactivate the block schedules. Please start planning now for surgeries/procedures (Clinic visits, STAR, Labs, Orders, Insurance Pre-auth, etc.). If you have any questions, please reach out to Dr. Jamie Park, Dr. Matt Mulder, Dr. Mike Burke or John Wagner.
Thank you for all your great work over the last few months!
Sincerely,
Jamie Park and Matt Mulder
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Dear Provider:
Thank you for your continued patience as we have worked through the circumstances of the past few months. The COVID outbreak has put most activities in our lives on hold. All of you have had to put off elective procedures and a big part of your practice. In part, this was to protect healthy folks from infection and to save our PPE and medical equipment for those who need it. We know that for your patients, waiting for an elective procedure can be fraught with anxiety and tension.
In total, VMC paused more than 2,000 surgeries and procedures out of an abundance of caution and concern for patient and employee safety, our uncertain PPE inventory and bed availability. Now, more than a month later, things have changed for the better. Our social interventions have helped flatten the curve. While we still need to follow our PPE conservation measures, we are in a better position to ensure sufficient supplies to take care of our patients. Evidence also indicates that the surge in COVID-19 cases in our communities has passed, giving us capacity to handle more surgeries and procedures.
Earlier this week, the governor issued updated guidance regarding the original proclamation in March. In summary it does two broad things:
- It further defines that urgent/emergent procedures should be based on a clinicians judgement in determining what cases should proceed (VMC has been following this logic)
- The second half discuss non-urgent case/elective cases. It describes that in the context of the current situation, providers should consider relative “harm” in delaying these cases and provides some practical definitions/guidance. Again, the governor is leaving the definition of “harm” up the individual clinician.
Importantly, it states that “The decision to perform any surgery or procedure in hospitals, ambulatory surgical facilities, dental, orthodontic, and endodontic offices, including examples of those that could be delayed in the Proclamation (i.e. total joints, some endoscopy, etc.), should be weighed against the following criteria when considering potential harm to a patient’s health and well-being”
Relative Harm Criteria:
• Expected advancement of disease process
• Possibility that delay results in more complex future surgery or treatment
• Increased loss of function
• Continuing or worsening of significant or severe pain
• Deterioration of the patient’s condition or overall health
• Delay would be expected to result in a less-positive ultimate medical or surgical outcome
• Leaving a condition untreated could render the patient more vulnerable to COVID-19 contraction, or resultant disease morbidity and/or mortality
• Non-surgical alternatives are not available or appropriate per current standards of care
• Patient’s co-morbidities or risk factors for morbidity or mortality, if inflicted with COVID-19 after procedure is performed
In summary and with this updated guidance in mind, the time has come to review all the delayed surgeries, procedures and diagnostic tests again. We have the ability to perform procedures safely for both our patients and staff. Please schedule any patient procedures which may include imaging, lab, interventional procedures and surgeries that in your clinical judgment you believe would cause your patients harm if further delayed. It’s important to note that proclamation and it’s requirements are still in effect until May 18.
ACTION ITEMS/NOTES:
- Any cases now deemed necessary should be scheduled through our normal process. This will allow us to get patients the care they need as soon as possible
- Please note that it’s critical that the clinical judgment supporting the scheduling and treatment determination should be documented in the patients record according to the criteria above through May 18.
- Dr. Molina has developed a dot phrase that must be used for all surgeries (except those coming through the ED) starting Monday, May 4. Please see here for instructions and content.
- Starting Wednesday May 6 through May 17, we will be expanding the number of rooms we are running to 8 per day. This will give us time to ramp up to the schedule starting May 18.
- On May 18, we intend on reactivating the granted block schedules. Please start planning ahead to schedule your surgeries (STAR Clinic, Labs, Orders, Insurance Pre-auth, etc.).
- Some blocks are moving to be auto released at 96 hours to ensure we minimize underutilized time—we will work to contact you/your office if impacted.
- All surgical/procedural patients will still need a COVID test 72 hours prior to their surgery—please continue the same practice. We are planning for the testing tent to open through at least June.
- Visitors will still be limited—all visitors will need to be screened and free of symptoms (fever, cough, SOB). Only one support person is allowed for peri-operative services.
- We will closely monitor our PPE, testing supplies and COVID-19 activity in our communities and facilities to ensure we are practicing as safely as possible. If we have a surge in COVID-19 activity that jeopardizes patient safety or PPE availability we will communicate appropriately as to any steps necessary to adjust our scheduling and treatment activities.
Post-Operative workflow
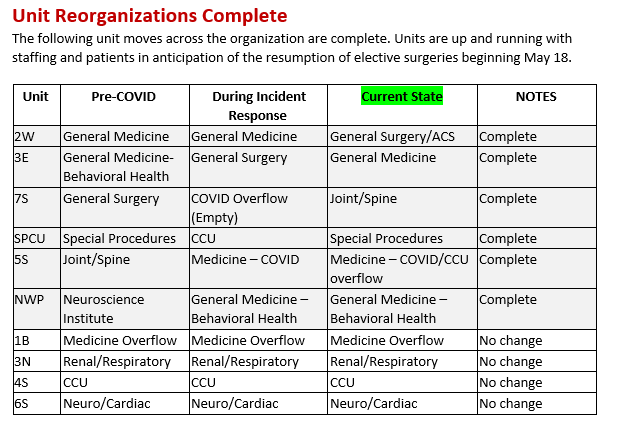
- As we strive to continue to respond to the COVID pandemic, we are making further unit changes that need to occur in order to serve our patients in the best way possible given our current unit and bed configurations. By implementing 5S as the COVID isolation unit, we eliminated one of our Surgical floors in the tower, and also closed 7S in case we saw an increase/surge of COVID patients that might need to be placed there. For this reason we opened 3East for surgical patients. However, as things ramp back up, we believe that we need another Surgery unit with greater bed occupancy as we strive to meet the demand and backlog of surgeries becoming increasingly urgent. Please note that appropriate staff will move to support these changes.
We are implementing the following:
- Relocating the 3 East surgery patients to 2 West. This will provide us much needed additional beds
- Joint and Spine Center will move to 7 South. This will provide the space and infrastructure to best support this patients populations needs.
- Please refer to the chart below for all unit reorganizations
Please share this information with others who need to be aware of this guidance. Thank you for your ongoing dedication and hard work during this uncertain time.